
“Top
surgery” is a common term for our Toronto transgender community, more specifically my female-to-male (FTM) patients. It refers to the removal of breast tissue and to the masculinization of their chest, a strong component o
f gender reassignment surgery.
I have been performing top plastic surgery here in Toronto since 2001.
I offer 6 different techniques of top surgery for my FTM transgender patients, of which there are 3 main versions. The choice of technique is not only dictated by the patient’s anatomy, but also by the patient’s choice of scar locations and the likelihood of a required second procedure, often called “second stage,” when discussing plastic reconstructive surgery.
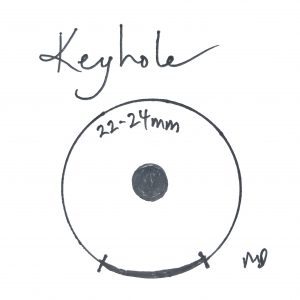
Drawings by Dr. Marc DuPéré
The simplest of all 3 techniques is the “keyhole” technique. The term is quite simple to understand for lay people as it refers to a “small opening”, i.e. a keyhole (yet confusing to inexperienced plastic surgeons as the keyhole technique in breast surgery refers to something else). This keyhole technique in masculinization of the chest refers to a small incision, between 5 and 7 o’clock at the areola’s border. The areola is the flat disk around the nipple. This technique was borrowed from our plastic surgery work on males with gynecomastia (breast tissue on males). Via this small incision at the brown-beige areolar line, most of the breast tissue can be removed. This technique is excellent for small breasts, small areolae, and young, elastic, and recoiling skin as no skin and no areolar tissue are removed. A strong advantage is most of the nipple feeling is preserved.

Dra
wings by Dr. Marc DuPéré
1 step up would be the “periareolar” or “donut” technique. I used this technique for moderate-sized breasts where there is a mild excess of skin to be excised along with small-to-moderate breast tissue. It is done via excision of a “donut-shaped” area of skin around the areola and closing it to a smaller “male-size” areola. There is a limit to the extra skin that can be removed with this technique, and therefore it works best for small-to-medium breasts. I sometimes use this technique for larger breasts when patients are very reluctant to do the under-the-breast incision of the double-incisio
n te
chnique; yet, a second-stage procedure is often required to deal with some mandatory residual breast tissue required to maintain the viability of the nipple-areolar complex with the mandatory long pedicles (as seen with larger and pendulous breasts). The final scar is a circle around the areola. Because a larger circle is closed to a smaller circle, there are commonly little folds around the areola that tend to efface and disappear over 1 to 3 months; otherwise, a small scar revision might be required. In this technique, if more skin is excised, the tension on the closure with various upper extremity movements is greater and the likelihood of scar widening is greater. If the amount of skin is lesser, then there might be some residual loose skin after surgery. So as an experienced plastic surgeon, I must determine the right balance of skin excision; the patient also knows that a revision might be required. Finally, because the nipple-areolar tissue is not completely severed, there is a very small possibility of maintaining some sensation.
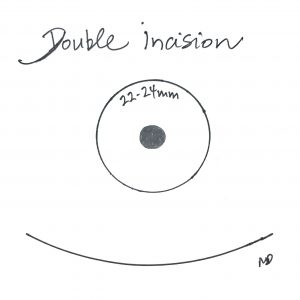
Drawings by Dr. Marc DuPéré
By far the most common technique is the so-called “double incision” technique. This is what I recommend for larger breasts. It allows for the removal of all breast tissue
and the resizing of the areola. Revisions are rare. The drawbacks are an incision in the small fold under the breasts and the time required for the new areola-nipple complexes to heal since those are grafted. The sexual feeling in the grafted nipples is also lost, but the “pressure” feeling and the ability to detect “cold/warm” usually returns to the nipples over time. The loss or necrosis of nipples (failed to “take” and heal) is possible but very rare.
A 4th technique would be liposuction alone, but it rarely provides an excellent masculine result.
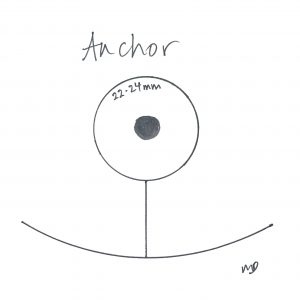
Drawings by Dr. Marc DuPéré
Finally, the old-style anchor reduction can be applied here too with complete excision of the breast tissue and preservation of a pedicled nipple-areolar complex. There is an added vertical scar which may seem very unsightly over the chest in a male. It is an “added” scar and does not serve many purposes over the double incision technique, except for the small theoretical chance of maybe saving some sensation to the nipple. I reserve this for patients who want to do anything to preserve some feeling, with large breasts and with hairy chest where the vertical incisions will be harder to see.
Adding a pectoral implant (a 6th procedure!) is another powerful procedure in masculinizing one’s chest. Pectoral augmentation will instantly give a patient’s chest a muscular, manly look. Pectoral implants can be added easily during “top surgery”, using either the conventional underarm incision or the IMF incision of the double incision technique.
In summary, TOP surgery is often the first procedure my FTM patients will undergo here in Toronto in their journey through gender reassignment. Following this, the next most common procedures will be masculinizing the face and the body, often with liposuction and etching, fillers to face, chin implant, jaw angle implants, calf implants, pectoral augmentation, etc.
If you have any questions or concerns, please contact us or call (416) 929-9800 (Yorkville) to book your first visit at Visage Clinic.
Dr. Marc DuPéré, Aesthetic, Cosmetic, and Plastic Surgeon




